
Written By:
Ali Le Vere, B.S., B.S. - Senior Researcher-Gre...

By now, I'm sure you've seen the USA Today article entitled, "Coconut oil isn't healthy. It's never been healthy". Fear-mongering, attention-grabbing headlines certainly sell copy, but do not make for evidence-informed, high quality science reporting.
As I expressed in my recent post on social media,
"The internet is full of erroneous claims. Science writers who forgo the nuances of empirical findings in the interest of sensational headlines.
False extrapolations made by people unequipped to interpret the research.Speculations by bloggers who missed the correlation-does-not-equal-causation lesson in epidemiology.
Over-generalizations from poorly designed, low quality in vitro and animal studies and studies that failed the test of statistical significance. Industry-funded, conflict-of-interest ridden rhetoric.
From eating for your blood type, to saturated fat causing heart disease, to heart-healthy whole wheat, to coffee causing gluten cross reactivity---in the natural and mainstream health communities alike, people take an idea and run with it without once going back to the primary and secondary literature to verify its scientific veracity.
The lack of scientific rigor that abounds in many corners of natural medicine is part of the reason that alternative medicine is marginalized by mainstream medicine. However, conventional medicine is equally culpable when it comes to its standards of care lacking a firm evidence-base.
I hope to fill this void, apply a scientific eye, and impart credence to therapeutic nutrition and holistic medicine by substantiating all my claims with high quality scientific data---instead of pulling statements out of thin air, which sadly is commonplace with headline-grabbing, yet substantive discussion-lacking online articles."
The USA Today article, written in response to an American Heart Association (AHA) statement advising Americans to replace saturated fat with omega-6 rich polyunsaturated fatty acids from vegetable oils, exemplifies the lack of journalistic integrity, rushing to conclusions, and flagrant misrepresentation of the data to which I was referring.
The Omega-3 to Omega-6 Ratio Determines Inflammatory Potential
Contrary to the implications of this USA Today piece, the evidence has elucidated that omega-6 fatty acids, which occur in the corn, cottonseed, canola, safflower, sunflower, and soybean oil that the AHA was recommending, promote carcinogenesis, whereas omega-3 fatty acids inhibit cancer development (Seaman, 2002). Hence, the Standard American Diet, rich in omega-6 fatty acid consumption, generates the pro-inflammatory state that facilitates tumorigenesis (Rose, 1997).
The detrimental effects of omega-6s are articulated by Fernandes and Venkatraman (1993), with,
“The increased consumption of many vegetable oils particularly of the n-6 series is…viewed as pro-inflammatory and is suspected as one of the possible causes for the rise in certain malignant tumors, rheumatoid arthritis and autoimmune diseases primarily due to the increased production of pro-inflammatory cytokines” (p. S19).
In contrast, long-chain omega-3 fatty acids from wild-caught fatty seafood, such as docosahexaenoic acid (DHA) can modify dynamics of the lipid bilayer, including elastic compressability and membrane permeability, promote membrane fluidity, and favorably modify membrane-bound protein activity (Stillwell & Wassall, 2003).
Thus, DHA is preventive in many inflammatory disorders, including cancer, cardiovascular disease, and neurodegenerative disease (Stillwell & Wassal, 2003). Specifically, DHA mitigates neuro-inflammation as it facilitates more efficient nerve cell communication (Crawford et al., 2013). The brains of patients with Alzheimer’s disease (AD) are deficient in DHA, and loss of structural and functional integrity of the brain correlates with loss of DHA concentrations in cell membranes in these patients (Seaman, 2002).
DHA and its long chain omega-3 precursor, eicosapentaenoic acid (EPA), are likewise involved in modulation of immune responses. In one study, supplementation of these fatty acids prolonged remission of systemic lupus erythematous (SLE) (Das, 1994). In another autoimmune disease, rheumatoid arthritis, omega-3 supplementation was found to suppress the production of inflammatory cytokines and eicosanoids involved in the pathogenesis of the disease (Morin, Blier, & Fortin, 2015). Mechanistically, long chain omega-3 fatty acids suppress proliferation of pathogenic T cells and inhibit synthesis of inflammatory cytokines such as tumor necrosis factor (TNF), interleukin-1 (IL-1), and interleukin-2 (IL-2) (Das, 1994).
The dietary balance of omega-6 to omega-3 fatty acids, which compete for incorporation into the phospholipid bilayer of cellular membranes, is integral for restoration of immune health and for prevention of long-latency, chronic, and degenerative diseases.
In order to generate optimal ratios of omega-6 to omega-3 fatty acids, ditch the toxic industrialized vegetable oils, and moderate consumption of grains and seeds as well, since they contain linoleic acid, the precursor to the omega-6 fatty acid arachidonic acid.
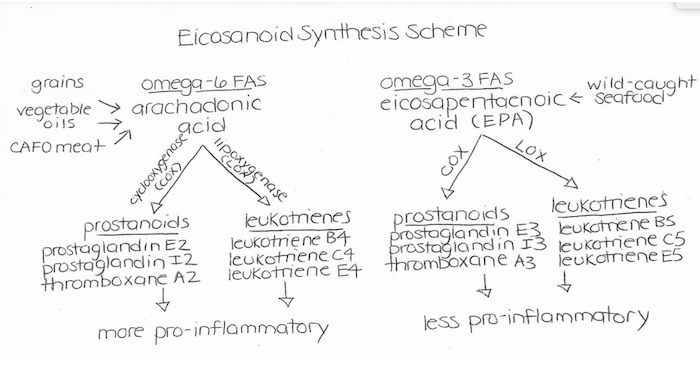
As I illustrated above, arachidonic acid is processed by the enzyme cyclooxygenase (COX) to produce pro-inflammatory signaling molecules called eicosanoids, including leukotrienes, prostaglandins, and thromboxanes. Omega-3 fatty acids, on the other hand, promote the production of less inflammatory mediators. Therefore, USA Today’s recommendation to increase consumption of pro-inflammatory vegetable oils, amidst an epidemic of inflammatory chronic diseases, is negligent and irresponsible.
Applying an Ethnographic and Evolutionary Biology Lens
Of all the diets, an ancestral paleolithic diet reminiscent of ancient foragers has the most optimal omega-6 to omega-3 ratio, of 1:1 (Simopoulos, 1991). Traditional hunter-gatherer cultures whose diets are composed of grass-fed game, pasture-raised poultry and eggs, wild-caught seafood, organic, local fruits and vegetables, roots and tubers, nuts and seeds are virtually free of the long-latency, degenerative diseases that plague Westerners.
Eskimos, for instance, who eat a high fish-based diet replete in omega-3s and very low in omega-6s, do not suffer from any of the diseases of modernity, including cancer, diabetes, heart disease, diverticulitis, appendicitis, gallstones, or autoimmune diseasessuch as multiple sclerosis, rheumatoid arthritis, psoriasis, or ulcerative colitis (Sinclair, 1981; Nettleton, 1995; Calder, 1998).
In contrast, the Standard American Diet, customary in Western cultures where non-communicable chronic diseases reach epidemic levels, has an omega-6 to omega-3 fatty acid ratio ranging from 10:1 to 25:1 (Simopoulos, 1991). This is largely due to the inclusion of pro-inflammatory, high-heat processed vegetable oils, which are subject to chemically-laden processes such as caustic refining, bleaching, and degumming, and then have to be chemically deodorized to negate rancidity.
In addition to minimizing vegetable oil intake, incorporating plenty of wild-caught, cold-water fatty fish, including mackerel, salmon, herring, caviar, and sardines, can enhance omega-3 levels. Crawford (1968) also demonstrated that wild animals eating their native diets have significantly more omega-3s compared to domesticated livestock. Grass-fed meat, for example, is replete in omega-3 fatty acids and antioxidants such as beta carotene and vitamin E compared to its conventional corn-fed counterparts, so incorporating grass-fed meat into your diet can restore balance in your fatty acid ratio (Daley et al., 2010).
Busting the Cholesterol Myth
Of note, is that the USA Today article vilified coconut oil on the basis that it raises LDL cholesterol. However, the most recent Dietary Guidelines Advisory Committee (DGAC) removed dietary cholesterol as a nutrient of concern, given that there is "no appreciable relationship between dietary cholesterol and serum cholesterol or clinical cardiovascular events in general populations,” so cholesterol content should not deter you from consumption of saturated fat (Mozaffarian & Ludwig, 2015, p. 2421).
Low total cholesterol, formerly believed to be protective against cardiovascular disease, has been demonstrated to have a litany of ill effects. In particular, women with a total cholesterol below 195 mg/dL have a higher risk of mortality compared to women with cholesterol above this cut-off (Petrusson, Sigurdsson, Bengtsson, Nilsen, & Getz, 2012).
Low cholesterol has been correlated with Alzheimer’s disease, dementia, suicide, homicide, accidental deaths, and morbid depression (Boscarino, Erlich, & Hoffman, 2009; Morgan, Palinkas, Barrett-Connor, & Wingard, 1993, Mielke et al., 2005; Seneff, Wainwright, & Mascitelli, 2011).
In a group of men 50 years and older, researchers found depression to be three times more common in the group with low plasma cholesterol (Morgan, Palinkas, Barrett-Connor, & Wingard, 1993). Shockingly, men with total cholesterol below 165 m/dL were also found to be seven times more likely to die prematurely from unnatural causes, including suicide and accidents (Boscarino, Erlich, & Hoffman, 2009).
In fact, Morgan, Palinkas, Barrett-Connor, and Winged (1993) articulate this with, “In several clinical trials of interventions designed to lower plasma cholesterol, reductions in coronary heart disease mortality have been offset by an unexplained rise in suicides and other violent deaths” (p. 75).
In essence, in progressive circles, the cholesterol-demonizing, artery-clogging model of heart disease has been redacted in favor of one where inflammation leads to endothelial and vascular smooth muscle dysfunction as well as oxidative stress. Like firefighters at a fire, cholesterol is present at the scene of the crime, but it is not the perpetrator---rather, it is a protective antioxidant element that repairs damage to arteries.
Moreover, cholesterol is an important precursor to our steroid hormones and bile acids, a membrane constituent that helps maintain structural integrity and fluidity, and an essential component for transmembrane transport, cell signaling, and nerve conduction.
Saturated Fat is Not Bad For You
Further, the recommendations of the AHA are especially surprising in light of the results of the Minnesota Coronary Experiment performed forty years ago, where the saturated fat in the diets of 9000 institutionalized mental patients was replaced with polyunsaturated fats in the form of corn oil. A 2010 re-evaluation of the data from this experiment was published in the British Medical Journal (Ramsden et al., 2016).
According to this re-analysis, these patients experienced a 22% higher risk of death for each 30 mg/dL reduction in serum cholesterol (Ramsden et al., 2016). Thus, although substituting omega-6 fats in place of saturated fat led to reductions in cholesterol, these patients suffered worse health outcomes, highlighting that cholesterol is not the villain it was formerly construed to be.
What's more, although the USA Today article declares the dangers of saturated fat, a recent meta-analysis in the American Journal of Clinical Nutrition, which compiled data from 21 studies including 347,747 people that were followed for an average of 14 years, concluded that there is no appreciable relationship between saturated fat consumptionand incidence of cardiovascular disease or stroke (Siri-Tarino, Sun, Hu, & Krauss, 2010).
Another meta-analysis published in 2015 in the British Journal of Medicine concluded that there is no association between saturated fat and risk of cardiovascular disease, coronary heart disease, ischemic stroke, type 2 diabetes, or all-cause mortality (the risk of death from any cause) (de Souza et al., 2015).
Along similar lines, a trial published in the American Journal of Nutrition in 2016 showed that eating a high fat diet, and deriving a large proportion of calories from saturated fat, improved biomarkers of cardiometabolic risk and insulin resistance, such as insulin, HDL, triglycerides, C-peptide, and glycated hemoglobin (Veum et al., 2016). The researchers conclude, "Our data do not support the idea that dietary fat per se promotes ectopic adiposity and cardiometabolic syndrome in humans" (Veum et al., 2016).
In actuality, saturated fat has been demonstrated to exert beneficial effects on levels of triglycerides and high-density lipoprotein cholesterol (HDL), the latter of which has been characterized as the "good cholesterol” that scavenges or transports cholesterol deposited in the bloodstream back to the liver (Mensink, Zock, Kester, & Katan, 2003). Saturated fat has also been shown to elicit minimal effects on apolipoprotein B, a risk factor for cardiovascular disease, relative to carbohydrates (Mensink, Zock, Kester, & Katan, 2003).
In addition, in a recent article in the Annals of Nutrition and Metabolism, an expert panel held jointly between the Food and Agriculture Organization (FAO) and World Health Organization (WHO) reviewed the relationship between saturated fat and coronary heart disease (CHD) (FAO/WHO, 2009).
From their examination of epidemiological studies, they found that saturated fatty acid intake was not significantly correlated with coronary heart disease events or mortality (FAO/WHO, 2009). Similarly, from their investigation of intervention studies, which are more powerful in that they can prove causality, they found that incidence of fatal coronary heart disease was not reduced by low-fat diets (FAO/WHO, 2009).
According to Mozaffarian and Ludwig (2015), "The 2015 DGAC report tacitly acknowledges the lack of convincing evidence to recommend low-fat–high-carbohydrate diets for the general public in the prevention or treatment of any major health outcome, including heart disease, stroke, cancer, diabetes, or obesity" (p. 2422).
Part of this reversal in guidelines is based on the fact that replacing protein or carbohydrates with healthy fats in excess of the current 35% of the daily caloric fat limit reduces risk of cardiovascular disease (Appel et al., 2005; Estruch et al., 2013).
In a similar vein, "The 2015 DGAC report specifies that, ‘Consumption of ‘low-fat’ or ‘nonfat’ products with high amounts of refined grains and added sugars should be discouraged’" (Mozaffarian & Ludwig, 2015, p.2422). Despite new guidelines, the Nutrition Facts Panel still employs the outdated 30% limit on dietary fat, which Mozaffarian and Ludwig (2015) remark has been "obsolete for more than a decade" (p.2422).
Coconut Oil Doesn’t Negate Health---It Engenders It
Not only do these meta-analyses put the nail in the coffin as far as saturated fat causing heart disease, but a plethora of health benefits have been elucidated in the scientific literature regarding coconut oil consumption. For instance, the following studies, as catalogued in the GreenMedInfo database, have revealed metabolic, immunomodulatory, and cognitive benefits of the dietary inclusion of coconut oil.
For instance, extra virgin coconut oil consumption has been demonstrated to significantly reduce body mass index (BMI) and waist circumference (WC) and produce significant increases in concentrations of HDL cholesterol in patients with coronary artery disease (CAD) (Cardoso et al., 2015). Another study by Liau in colleagues (2011) concluded that virgin coconut oil is efficacious for the reduction of waist circumference, especially in a male cohort. Likewise, a study by Assunção and colleagues (2009) demonstrated that dietary coconut oil reduces visceral adiposity and elevates HDL cholesterol in women, thus improving both anthropometric and biochemical risk factors for metabolic syndrome.
In rodent models, dietary virgin coconut oil improves glycemic control in high fructose fed rats, and is postulated to be “an efficient nutraceutical in preventing the development of diet induced insulin resistance and associated complications possibly through its antioxidant efficacy” (Narayanankutty et al., 2016). Research supports the use of coconut oil for obesity, dyslipidemia, insulin resistance, hypertension, and pathologically elevated LDL, all of which constitute risk factors for diabetes, cardiovascular disease, and Alzheimer’s, the last of which is being re-conceptualized as type 3 diabetes (Fernando et al., 2015).
In addition, in a prospective study of patients with Alzheimer’s, improvements in cognitive function were observed for patients administered extra virgin coconut oil, since “medium chain triglycerides are a direct source of cellular energy and can be a nonpharmacological alternative to the neuronal death for lack of it, that occurs in Alzheimer patients” (Yang et al., 2015). Notably, the hormones, or cytokinins, and phenolic compounds found in coconut may prevent aggregation of amyloid-β peptide into plaques, thus arresting a critical step in pathogenesis of Alzheimer’s (Fernando et al., 2015). Research also suggests that coconut oil may directly stimulate ketogenesis in astrocytes and provide fuel to neighboring neurons as a consequence, thus improving brain health (Nonaka et al., 2016). On a different note, coconut oil mitigates amyloid beta toxicity in cortical neurons by up-regulating signaling of cell survival pathways (Nafar, Clarke, & Mearow, 2017).
Lastly, studies have illuminated anti-inflammatory, analgesic, antibacterial, and anti-pyretic properties of virgin coconut oil (Intahphuak, Khonsung, & Panthong, 2010; Ogbolu et al., 2007). Thus, unless you are part of the minority of the population that carries the APOE4 allele, a polymorphism that confers increased risk with saturated fat consumption, there is no reason to avoid coconut oil or saturated fat (Barberger-Gateau et al., 2011). Thus, instead of trashing your coconut oil, do yourself a favor and eat an extra helping---your body will thank you.
For evidence-based reseach on coconut oil, visit the GreenMedInfo.com Research Dashboard.
References
Appel, L.J., Sacks, F.M., Carey, V.J., Obarzanek, E. Swain, J.F., Miller, E.R. 3rd,...OmniHeart Collaborative Research Group. (2005). Effects of protein, monounsaturated fat, and carbohydrate intake on blood pressure and serum lipids: results of the OmniHeart randomized trial. Journal of the American Medical Association, 294(19):2455-2464.
Assunção, M.L., Ferreira, H.S., dos Santos, A.F., Cabral, C.R., & Florêncio, T.M.M.T. (2009). Effects of dietary coconut oil on the biochemical and anthropometric profiles of women presenting abdominal obesity. Lipids, 44(7), 593-601.
Barberger-Gateua, P., Samieri, C., Feart, C., & Plourde, M. (2012). Dietary omega 3 polyunsaturated fatty acids and Alzheimer’s disease: interaction with apolipoprotein E genotype. Current Alzheimer’s Research, 8(5), 479-491.
Calder, P.C. (1998). Dietary fatty acids and the immune system. Nutritional Reviews, II, S70-S83.
Cardoso et al. (2015). A coconut extra virgin oil-rich diet increases HDL cholesterol and decreases waist circumference and body mass in coronary artery disease patients. Nutrition Hospitals, 32(5), 2144-2152. doi: 10.3305/nh.2015.32.5.9642.
Crawford, M.A., Broadhurst, C.L., Guest, M., Nagar, A., Wang, Y., Ghebremeskel, K., & Schmidt, W. (2013). A quantum theory for the irreplaceable role of docosahexaenoic acid in neural cell signaling throughout evolution. Prostaglandins Leukotrienes and Essential Fatty Acids, 88(1), 5-13.
Daley, C. A., Abbott, A., Doyle, P. S., Nader, G. A., & Larson, S. (2010). A review of fatty acid profiles and antioxidant content in grass-fed and grain-fed beef. Nutrition Journal, 9(1), 10.
Das, U.N. (1994). Beneficial effect of eicosapentaenoic and docosahexaenoic acids in the management of systemic lupus erythematosus and its relationship to the cytokine network. Prostaglandins Leukotrienes and Essential Fatty Acids, 51(3), 207-213.
de Souza et al. (2015). Intake of saturated and trans unsaturated fatty acids and risk of all cause mortality, cardiovascular disease, and type 2 diabetes: a systematic review and meta-anlaysis of observational studies. British Medical Journal, 351.
Estruch, R., Ros, E., Salas-Salvado, J., Covas, M.I., Corella, D., Aros, F.,...PREDIMED Study Investigators. (2013). Primary prevention of cardiovascular disease with a Mediterranean diet. New England Journal of Medicine, 368(14), 1279-1290. doi: 10.1056/NEJMoa1200303
FAO/WHO. (2009). Fats and fatty acids in human nutrition. Proceedings of the Joint FAO/WHO Expert Consultation. November 10-14, 2008. Geneva, Switzerland. Annals of Nutrition and Metabolism, 55, 1-3.
Fernando, W.M.A.D.B., Martins, I.J., Goozee, K.G., Brennan, C.S., Jayasena, V., & Martins, R.N. (2015). The role of dietary coconut for the prevention and treatment of Alzheimer's disease: potential mechanisms of action. British Journal of Nutrition, 1-14.
Intahphuak, S., Khonsung, P., & Panthong, A. (2010). Anti-inflammatory, analgesic, and antipyretic activities of virgin coconut oil. Pharmacological Biology, 48(2), 151-157.
Kalmijn, S., Feskens, E.J.M., & Kromhout, D. (1997). Polyunsaturated fatty acids, antioxidants, and cognitive function in very old men. American journal of Epidemiology, 145, 33-41.
Liau, K.M., Lee, Y.Y., Chen, C.K., & Rasool, A.H.G. (2011). An open-label pilot study to assess the efficacy and safety of virgin coconut oil in reducing visceral adiposity. ISRN Pharmacology. doi: 10.5402/2011/949686
Mensink, R.P., Zock, P.L., Kester, A.D., & Katan, M.B. (2003). Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: a meta-analysis of 60 controlled trials. American Journal of Clinical Nutrition, 77(5), 1146-1155.
Mielke, M.M., Zandi, P.P., Sjogren, M., Gustafson, D., Ostling, S., Steen, B., & Skoog, I. (2005). High total cholesterol levels in late life associated with a reduced risk of dementia. Neurology, 64(10), 1689-1695.
Mozaffarian, D., & Ludwig, D.S. (2015). The 2015 US Dietary Guidelines: Lifting the Ban on Total Dietary Fat. Journal of the American Medical Association, 313(24), 2421-2422.
Morin, C., Blier, P.U., & Fortin, S. (2015). Eicosapentaenoic acid and docosapentaenoic acid monoglycerides are more potent than docosahexaenoic acid monoglyceride to resolve inflammation in a rheumatoid arthritis model. Arthritis Research Therapies, 17, 142. doi: 10.1186/s13075-015-0653-y.
Morgan, R.E., Palinkas, L.A., Barrett-Connor, E.L., & Wingard, D.L. (1993). Plasma cholesterol and depressive symptoms in older men. The Lancet, 341(8837), 75-79. doi:10.1016/0140-6736(93)92556-9
Nafar, F., Clarke, J.P., & Mearow, K.M. (2017). Coconut oil protects cortical neurons from amyloid beta toxicity by enhancing signaling of cell survival pathways. Neurochemical International, 105, 64-79. doi: 10.1016/j.neuint.2017.01.008.
Narayanankutty, A., Mukesh, R.K., Ayoob, S.K., Ramavarma, S.K., Suseela, I.M., Manalil, J.J.,…Raghavamenon, A.C. (2016). Virgin coconut oil maintains redox status and improves glycemic conditions in high fructose fed rats. Journal of Food Science and Technology, 53(1), 895-901.
Nettleton, J. (1995). omega-3 fatty acids and health. New York Chapman & Hall. p. 67-73.
Nonaka, Y., Takagi, T., Inai, M., Nishimura, S., Urashima, S., Honda, K.,…Terada, S. (2016). Lauric acid stimulates ketone body production in the KT-5 astrocyte cell line. Journal of Oleo Science, 65(8), 693-699.
Ogbolu, D.O., Oni, A.A., Daini, O.A., & Oloko, A.P. (2007). In vitro antimicrobial properties of coconut oil on Candida species in Ibadan, Nigeria. Journal of Medical Foods, 10(2), 384-387.
Petrusson, H., Sigurdsson, J.A., Bengtsson, C., Nilsen, T.I., & Getz, L. (2012). Is the use of cholesterol in mortality risk algorithms in clinical guidelines valid? Ten years prospective data from the Norwegian HUNT 2 study. Journal of the Evaluation of Clinical Practice, 18(1), 159-168.
Ramsden et al. (2016). Re-evaluation of the traditional diet-heart hypothesis: analysis of recovered data from Minnesota Coronary Experiment (1968-1973). British Medical Journal, 353.Simopoulos, A.P., & Salem Jr., N. (1992). Egg yolk as a source of long-chain polyunsaturated fatty acids in infant feeding. American Journal of Clinical Nutrition, 55, 411-414.
Rose, D.P. (1997). Dietary fatty acids and cancer. American Journal of Clinical Nutrition, 66(suppl), 998S-1003S.
Seaman, D.R. (2002). The diet-induced pro-inflammatory state: a cause of chronic pain and other degenerative diseases? Journal of Manipulative and Physiological Therapeutics, 25(3), 168-179.
Seneff, S., Wainwright, G., & Mascitelli, L. (2011). Nutrition and Alzheimer’s disease: The detrimental role of a high carbohydrate diet. European Journal of Internal Medicine, 1-7.
Simopoulos, A.P. (1991). Omega-3 fatty acids in health and disease and in growth and development. American Journal of Clinical Nutrition, 54, 483-463.
Sinclair, H. (1981). The relative importance of essential fatty acids of the linoleum and linolenic families: studies with an Eskimo diet. Progress in Lipid Research, 20, 897-899.
Siri-Tarino, P.W., Sun, Q., Hu, F.B., & Krauss, R.M. (2010). Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease. American Journal of Clinical Nutrition, 91(3), 535-546.
Stillwell, W., & Wassall, S.R. (2003). Docosahexaenoic acid: membrane properties of a unique fatty acid. Chemistry and Physical Lipids, 126(1), 1-27.
Veum et al. (2016). Visceral adiposity and metabolic syndrome after very high-fat and low fat isocaloric diets: a randomized controlled trial. American Journal of Clinical Nutrition. doi: 10.3945/ajcn.115.123463
Yang, H.Y., de la Rubia Orti, J.E., Sabater, P.S., Castillo, S.S., Rochina, M.J., Ramon, N.M., & Montoya-Castilla, I. (2015). Coconut oil: Non-alternative drug treatment against Alzheimer’s disease. Nutrition in Hospitals, 32(6), 2822-2877.

Ali Le Vere holds dual Bachelor of Science degrees in Human Biology and Psychology, minors in Health Promotion and in Bioethics, Humanities, and Society, and is a Master of Science in Human Nutrition and Functional Medicine candidate. Having contended with chronic illness, her mission is to educate the public about the transformative potential of therapeutic nutrition and to disseminate information on evidence-based, empirically rooted holistic healing modalities. Read more at @empoweredautoimmune on Instagram and at www.EmpoweredAutoimmune.com: Science-based natural remedies for autoimmune disease, dysautonomia, Lyme disease, and other chronic, inflammatory illnesses.
Article by: Ali Le Vere (http://www.greenmedinfo.com/blog/defense-coconut-oil-rebuttal-usa-today)